|
October 2000
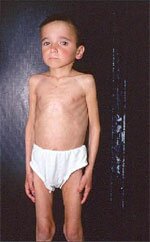
Case of the Month: This 10-year-old HIV-infected boy has had a 4-kg weight loss over the past two months. He denies nausea, vomiting or diarrhea, and has no fever. His current weight and height are 21 kg and 130 cm, respectively.
Diagnosis: Wasting
Discussion: Wasting is defined as the following in the absence of a concurrent illness other than HIV: (1) persistent weight loss >10% of baseline; (2) downward crossing of two or more major percentile lines on the pediatric weight-for-age chart (e.g., 95th, 75th, 50th, 25th, 5th); or (3) <5th percentile on weight-for-height chart on two consecutive measurements 30 or more days apart, plus chronic diarrhea or documented fever.
This patient has lost 19% of his body weight and has crossed two major percentile lines on the weight-for-age chart. His height-for-age and weight-for- height fall at the 10th and below the 3rd percentile, respectively. His BMI (body mass index: kg/m2), at 12.4, indicates growth failure as well. (Go to www.cdc.gov/growthcharts/ for the latest pediatric growth charts.)
The Waterlow criteria define stages of acute and chronic nutritional status based on weight-for-height and height-for-age (Waterlow, JC. Classification and definition of protein-calorie malnutrition. Brit Med 3:566, 1972). This child’s ideal body weight (IBW) for height is 27 kg, so he is at 77% or Stage II (moderate) acute malnutrition according to the Waterlow criteria. Also according to the Waterlow criteria, his chronic nutritional status, based on current length versus length-for-age at the 50th percentile, is at 94% or Stage I (mild) chronic malnutrition.
Loss of lean body mass or wasting is a well-recognized AIDS-defining condition for children and adults. HIV infection per se, as well as opportunistic infections, increase metabolic demands, leading to loss of weight and lean body mass. In children, wasting can severely impact normal growth and development. Also, wasting is associated with high risk for HIV disease progression and short-term mortality. For these reasons, it is important to prevent or reverse malnutrition and wasting.
Intervention: Effective antiretroviral therapy is key to preventing or reversing wasting. A three-day calorie count or a 24-hour diet recall can help in assessing the child’s current calorie and protein intake. HIV infection increases calorie needs to at least 150% of the U.S. Recommended Dietary Allowance for age. Protein intake can be increased to 4 gm/kg/day. A method to determine calorie needs is:
RDA calories for age x IBW / current weight
For example:
70 (RDA calories) x 27(IBW)/ 21(current weight) = 90 calories/kg/day
For protein the formula is the same, substituting RDA for protein instead of calories:
1.0g(RDA protein) x 27(IBW)/ 21(current weight) = 1.3g pro/kg/day
These calculations are starting points to determine needs for weight gain and growth. A high calorie, high protein diet, together with highly active antiretroviral therapy, should promote weight gain and growth. Because HIV infection increases micronutrient needs, a multiple vitamin and mineral supplement of at least 100% of the RDA, should also be given. Regular evaluations for medication adherence, and serial measurements of height and weight, are vital.
|
